




증례
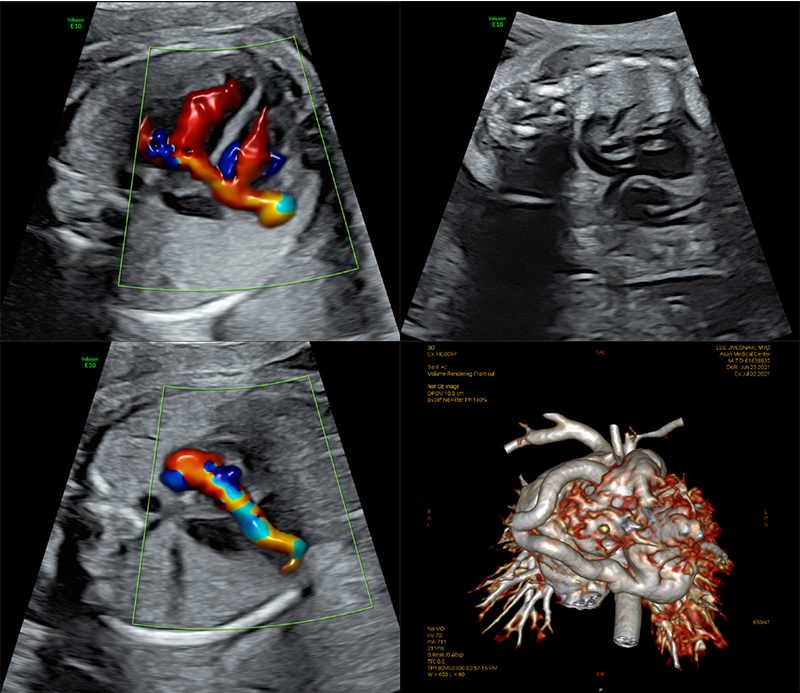
26주에 ventricular septal defect 의심되어 전원 되었음.
(A) 4 chamber view에서 color Doppler상 오른쪽에서 왼쪽으로 흐르는 비정상적인 flow가 관찰되었음.
(B) 대동맥에서 분지된 right coronary artery (RCA)가 비정상적으로 늘어나 있었음.
(C) RCA를 tracing하였을 때 심장의 inferior wall로 돌아가 left ventricle (LV)과 연결되는 소견이 관찰됨.
(D) 출생 후 Cardiac CT에서 RCA와 LV inferior wall 사이에 fistula가 확인되어 patch closure 시행함.
무심장 쌍태아(acardiac twin)의 성공적인 보존적 치료 최윤선(성균관의대 삼성서울병원 전공의)
무심장 쌍태아(acardiac twin)는 역전동맥관류 (twin reversed-arterial perfusion sequence)에 의하여 단일 양막성 쌍태아에서 발생하는 드문 합병증으로 분만 35,000건당 1명 꼴로 발생한다 [1]. 산전 진단은 초음파로 가능하며, 공여 태아의 생존율을 높여주기 때문에 조기 진단하는 것이 중요하다.
이 증례는 35세 초임부로, 2차례 유산 후 4번의 체외수정으로 단일 융모막 쌍태아를 임신했으며, 임신 12주 쌍둥이 소실(vanishing twin)을 진단받았다. 이후 추적관찰 중 유산된 태아가 크기가 점점 커지며 움직임이 있다는 소견으로 임신 27주에 본원으로 전원되었다. 본원에서 시행한 정밀초음파에서 21cm 크기의 무심장 쌍태아가 진단되었고, 공여 태아는 특별한 이상소견이 없었다 (그림1). 무심장 쌍태아의 탯줄 동맥의 색 도플러에서는 역전 동맥 관류(reverse arterial flow)가 확인되었다 (그림2). 산모는 36주까지 주 1회 초음파 추적검사를 시행했으며, 공여 태아는 태아수종, 심부전, 성장제한 등의 이상소견을 보이지 않았다. 임신 37주 선택적 제왕절개 수술을 시행했으며, 공여 태아는 여아 2.73kg으로 출생 후 적혈구증가증을 진단 받아 부분교환수혈을 받은 후 안정적으로 퇴원했다. 무심장 쌍태아는 여아 3.21kg로 목에서 천골까지 낭성 종괴가 확인되었고, 내반족(club foot)이었으며, 발가락은 양측 모두 4개씩만 있는 육안적 소견을 보였다 (그림 3).
참고문헌
- Chanthasenanont, A. and D. Pongrojpaw, Acardiac twin. J Med Assoc Thai, 2005. 88(11): p. 1721-4.
- Kariappa, T.M., H.T. Chidananda, and R. Mamatha, Acardiac twin: an unusual case report. Indian J Pathol Microbiol, 2007. 50(4): p. 801-3.
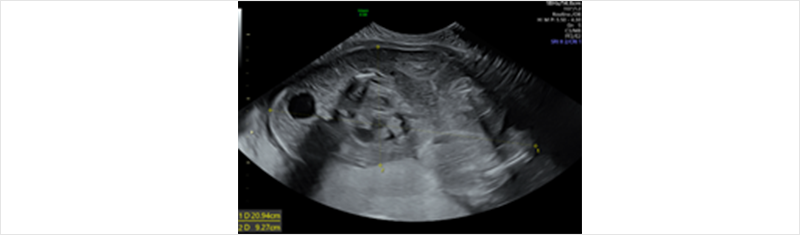 그림 1. 27주 발견한 21cm 크기의 무심장 쌍태아
그림 1. 27주 발견한 21cm 크기의 무심장 쌍태아
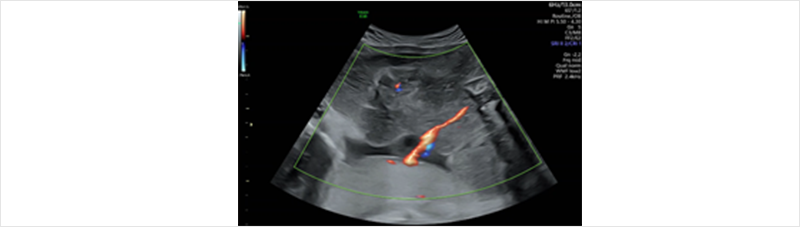 그림 2. 무심장 쌍태아를 향하는 역전 동맥 관류 (임신 27주 사진)
그림 2. 무심장 쌍태아를 향하는 역전 동맥 관류 (임신 27주 사진)
![[figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.](/webzine/2022vol1/image/sub/sub9_img10.png) 그림 3. 37주 제왕절개로 분만된 무심장 쌍태아의 육안 소견
그림 3. 37주 제왕절개로 분만된 무심장 쌍태아의 육안 소견
본 증례는 2021월 11월 5일 개최된 제 24차 대한산부인과초음파학회 추계학술대회 Image Contest에서 발표된 내용입니다.
![[figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.](/webzine/2022vol1/image/sub/sub9_img01.png) [figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.
[figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.
![[figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.](/webzine/2022vol1/image/sub/sub9_img02.png) Figure 2. MRI at pregnancy 14+4 weeks. Well-defined multicystic appearance in the placenta of
Figure 2. MRI at pregnancy 14+4 weeks. Well-defined multicystic appearance in the placenta of smaller fetus(about 10cm extent)
![[figure 1] cervix canal 주변에 2*1cm sized hypoechoic lesion 관찰됨.](/webzine/2022vol1/image/sub/sub9_img03.png) Figure 3. Histologic finding of Placental mesenchymal dysplasia. Edematous stem villi,
Figure 3. Histologic finding of Placental mesenchymal dysplasia. Edematous stem villi, thick-walled blood vessel are typical histologic finding of Placental mesenchymal dysplasia.
(1) 발표자: 조수빈 (연세의대)
(2) 제목: Cervical arteriovenous malformation during pregnancy
(3) 설명
33-year-old , Gravida 1, para0
PHx: 과거 교통사고로 인한 골반 골절 및 다발성 장기 손상되어 cystostomy, illeostomy, vaginal stenosis, s/p kidney transplantation, s/p appendicovesicostomy 받았었음.
IUP at 15weeks sono 상 cervix canal 주변에 다량의 혈류가 관찰되는 2*1cm sized hypoechoic lesion 관찰되어 cervical arteriovenous malformation 진단되었음. 질 출혈은 발생하지 않았지만 심한 빈혈 발생하여 수혈 진행하면 경과 관찰 중 임신 25주 0일 심한 질출혈 발생하며 Hemoglobin 3.3 g/dL 확인되어 수혈하며 경과 관찰하였으나, 25주 3일 심한 질출혈이 재발생하여 cervical arteriovenous malformation 의 active bleeding 소견으로 응급 제왕절개술 시행하였음. 수술 후 1일차에 복부 CT 촬영하였으며, 자궁과 자궁경부 주변에서 engorged vessel 외 bleeding 소견은 관찰되지 않았으며, 산모는 합병증 없이 퇴원하였음. 출생아는 710gm 남아로 아프가 점수 1분 2점, 2분 5점이었고 prematurity로 NICU 입원하여 보존적 치료 중임.
A 34 year-old woman with 11+3 gestational weeks was referred to our hospital because of 3.0mm of 2nd baby's nuchal translucency. The prenatal ultrasonography of 2nd baby showed multicystic appearance(Figure 1). We took Pelvic MRI at 14+4 weeks of gestation because we couldn’t rule out H-mole(Figure 2). About 10cm extent well-defined multicystic appearance was seen in the placenta of smaller baby and there's no evidence of deep myometrial invasion, extrauterine soft tissue infiltration, and hemorrhage. We referred her to other hospital and she got amniocentesis at 16 weeks of gestation at other hospital. Both baby's karyotype, chromosome test result were non-specific. Serum b-hCG level was 79,200 at 16+3 weeks of gestation.
From theses results, H-mole was ruled out and she was referred to our hospital again and elective cesarean section was done at 37+1 weeks of gestation. 1st baby was 2,370g, her apgar score was 10(1 minute), 10(5 minute). 2nd baby who was thought to be molar pregnancy was 2120g(IUGR) and her apgar score was 7(1 minute), 9(5 minute). Later biopsy result of 2nd baby's placenta was placental mesenchymal dysplasia(Figure 3).
Placental mesenchymal dysplasia is similar with molar pregnancy because of its cystic structure, enlarged uterus and placentomegaly. In this case, the facts that 2nd baby's normal karyotype, disappeared cystic pattern of placenta at 32+3 gestation weeks stand for placental mesenchymal dysplasia rather than molar pregnancy. In order to prevent unnecessary abortion, we must differentiate placental mesenchymal dysplasia from molar pregnancy appropriately. Histologically, the involvement of stem rather than terminal villi and lack of trophoblast proliferation distinguish placental mesenchymal dysplasia from H-mole.
 Figure 1. Ultrasonography at pregnancy 11+3 weeks, 2nd baby’s placenta shows multicystic appearance
Figure 1. Ultrasonography at pregnancy 11+3 weeks, 2nd baby’s placenta shows multicystic appearance
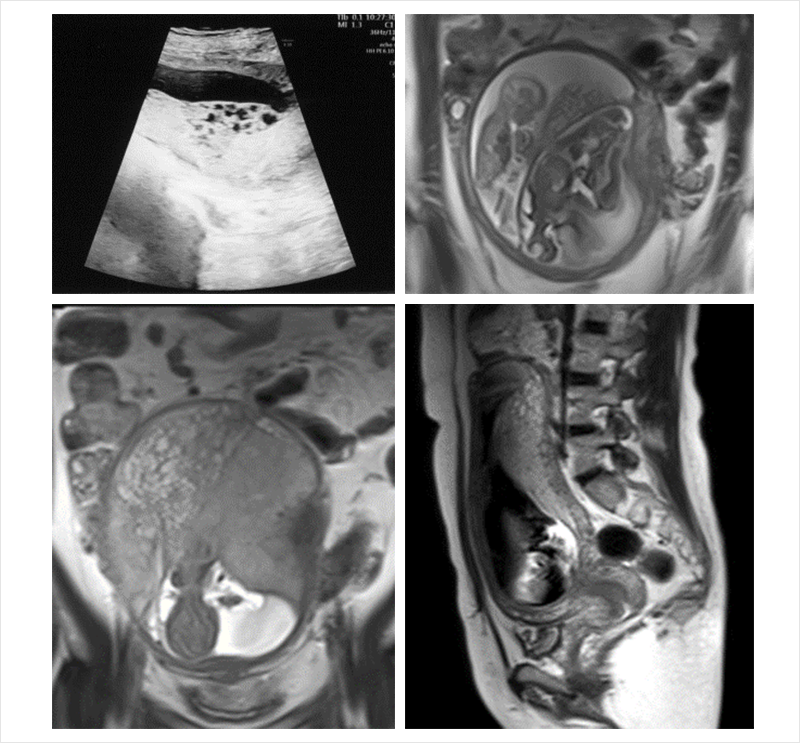 Figure 2. MRI at pregnancy 14+4 weeks. Well-defined multicystic appearance in the placenta of smaller fetus(about 10cm extent)
Figure 2. MRI at pregnancy 14+4 weeks. Well-defined multicystic appearance in the placenta of smaller fetus(about 10cm extent)
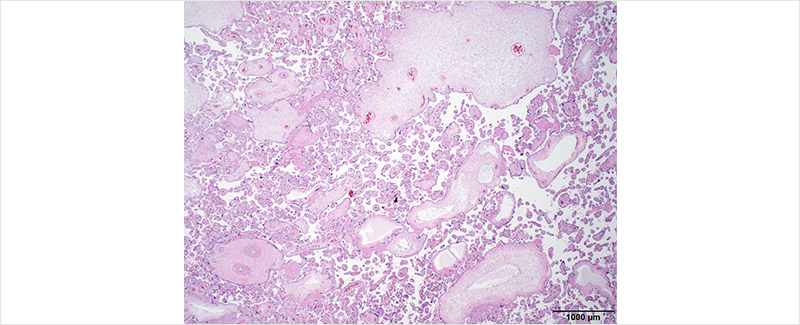 Figure 3. Histologic finding of Placental mesenchymal dysplasia. Edematous stem villi, thick-walled blood vessel are typical histologic finding of Placental mesenchymal dysplasia.
Figure 3. Histologic finding of Placental mesenchymal dysplasia. Edematous stem villi, thick-walled blood vessel are typical histologic finding of Placental mesenchymal dysplasia.